Pregnancy
The Spanish Society of Gynecology and Obstetrics (SEGO) and the Spanish Society of Periodontology and Osseointegration (SEPA) drafted a report that we summarize here so that you are up to date with the most important measures regarding your oral health during pregnancy.
The behavior of periodontal tissues can vary depending on changes in hormonal levels experienced at different stages and circumstances of a person's life.
Pregnancy is known for being the period in which the greatest physiological hormonal changes occur in a woman's life. One of the areas of the body most affected by these changes is the mouth, so these changes and their repercussions should be understood by the various professionals who care for women before and during pregnancy.
Hormonal variations are capable of inducing changes in the response of periodontal tissues because periodontal homeostasis is related to the endocrine system in a complex and multifactorial manner. The main effect observed is an increase in the gingival inflammation without any changes in the amount of bacterial plaque present.
Additionally, during pregnancy there is greater susceptibility to infections, meaning there is a greater likelihood of contracting an infection, such as gum disease.
Given the strong relationship between oral hygiene conditions and overall health, oral health itself should be a right for everyone.
However, if scientific evidence suggests that maternal periodontal disease may be a risk factor for premature birth, both education and oral hygiene measures should be especially targeted toward pregnant women.
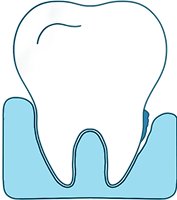
Pregnancy gingivitis
During pregnancy, an increase in gingival inflammation is observed, with a maximum peak in the second and third trimester compared to non-pregnant or postpartum women.
Associated clinical signs are:
- Presence of plaque on the gingival margin.
- Pronounced gingival inflammatory response.
- Establishment during pregnancy (2nd or 3rd trimester)
- Changes in gingival color or contour.
- Bleeding on probing.
- Reversible after delivery
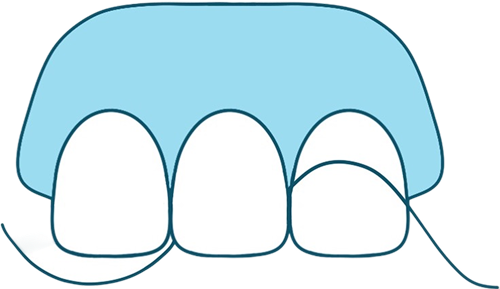
Pregnancy periodontitis
Recent studies indicate that periodontal destruction may increase during pregnancy. However, although studies indicate that this increase in probing depth appears to be due to inflammatory changes in the gingiva, it should be noted that these changes can establish very favorable conditions for the development and growth of periodontal bacteria, which can lead to increased periodontal disease activity.
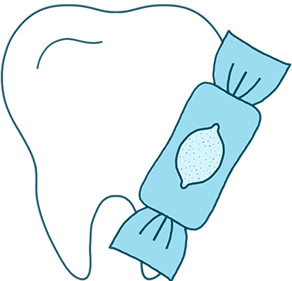
Cavities in pregnancy
During pregnancy, a worsening of pre-existing caries has been observed due to the following factors:
- Nutritional changes, such as changes in dietary habits, with a greater tendency toward sweet foods and snacking.
- Estrogens modify salivary peroxidases, which are active against various microorganisms.
- Changes in oral hygiene habits, which can be hampered by nausea, which can occur in up to 80% of pregnant women.
- During pregnancy, significant changes in behavior can occur, which can also affect oral hygiene habits.
- Vomiting, common in the first trimester of pregnancy, promotes tooth demineralization due to its acidity.
Early diagnosis of dental caries during pregnancy is essential, since early enamel lesions can be treated noninvasively by remineralization.
Premature birth
A relationship has been observed between periodontitis and premature births (37 days before the due date and low neonatal weight).
The presence of Porphyromonas gyngivalis has been demonstrated in placental tissue.This bacteria is directly linked to periodontal disease. It's a sign that these bacteria can cross the placental barrier and produce toxins. The body responds by producing inflammatory substances, causing increased physical stress to the point of premature birth.
Maternal infections are one of the main causes of premature birth, with ascending infections (from the vagina) being one of the most important etiological factors for prematurity in early pregnancy. So much so that almost 75% of premature births and very low birth weight fetuses are due to them.
Despite the proven relationship between maternal infection and premature birth, in more than 50% of cases the causes of prematurity are unknown, which is why the search for other etiological factors continues to be emphasized, among which, an important place is occupied by oral infections and, among them, periodontal infections of the mother, such as chronic infections, could represent a risk for the appearance of these problems.
Preeclampsia
Preeclampsia is a multisystem syndrome specific to human pregnancy, which develops as a result of systemic endothelial dysfunction, manifesting from 20th week of gestation WITH hypertension and proteinuria.
Despite the advances made in recent years in perinatal medicine, it remains one of the leading causes of maternal mortality and morbidity worldwide, especially in severe and/or early cases, accounting for 15% of pregnancy-related maternal deaths.
Preeclampsia is also an important cause of perinatal morbidity and mortality due to its association with placental abruption, intrauterine growth restriction, and premature birth.
Its etiology is multifactorial and diagnosis is based on clinical manifestations, since no specific test is yet available for its diagnosis.
Recent studies have linked the Periodontitis as a risk factor for preeclampsia, based on the fact that the systemic inflammation it produces releases high levels of C-reactive protein, cytokines and PGE2, which could cause pathophysiological changes in the uterine-placental circulation and lead to placental insufficiency and ischemia.
Although the results are not conclusive given the different methodologies used in the studies, systematic reviews and meta-analyses suggest that periodontitis may be a risk factor for developing preeclampsia.
Prevention
It is advisable to prevent and see a dentist before pregnancy, but it can also be treated during pregnancy, since many women experience a worsening of the problem once they become pregnant. It is important to treat this problem because if it worsens, more and more bacteria enter the bloodstream and this is what affects the fetus.
To facilitate prevention and ensure greater confidence in the condition of your gums, there is a guideline test that can be completed at cuidatusencias.es
Treatment
Fifty percent of pregnant women suffer from gingivitis and 10% from periodontitis. Treating it is vitally important to reduce the risk to the fetus and prevent infections. During pregnancy, the necessary treatments can be administered to resolve the problem. We must work closely with other specialists, such as gynecologists, who can verify what type of antibiotics are recommended, if necessary.
Second quarter
Various studies show that both dental and periodontal treatment performed during the second trimester (between weeks 13 and 21 of gestation) are not associated with an increased risk of adverse medical events or adverse outcomes during pregnancy.
The reasons for performing surgery at this stage of pregnancy are because organogenesis (the formation of fetal organs) has completed, and there's also a lower risk of miscarriage. In addition, the woman will experience less nausea and be more comfortable in the dental chair.
Antibiotics
Regarding the use of antibiotics, periodontitis does not always require treatment with these medications, except in very advanced cases. Gynecologists confirm that antibiotics such as amoxicillin, amoxicillin with clavulanic acid, azithromycin, clindamycin, gentamicin, erythromycin, clarithromycin, penicillin, cefazolin, cefotaxime, ceftriaxone, cefuroxime axetil, cefixime, cefoxitin, and aztreonam can be used.
Regarding metronidazole, it should be administered with caution. The risk/benefit ratio must be assessed during pregnancy.